
From the 1U1179 INSERM, University of Versailles Saint Quentin en Yvelines, Montigny le Bretonneux, 2Orthopedic Surgery Department, Raymond Poincaré Hospital, Garches, 3Radiotherapy Department, René Huguenin Hospital, Saint Cloud, and 4Department of Physical and Rehabilitation Medicine, U1228 - University of Rennes 1, Pontchaillou Hospital, Rennes, France
Objective: To evaluate recurrence and early post-operative complications (sepsis) following surgical excision combined with radiotherapy for trouble-some hip heterotopic ossification in patients with spinal cord injury and traumatic brain injury.
Design: Retrospective case-control study.
Setting: Data relating to patients with spinal cord injury or traumatic brain injury who underwent surgical excision of hip heterotopic ossification were retrieved from the BANKHO database. Case patients underwent excision + radiotherapy, and controls underwent excision only. Control patients were matched to case patients according to sex and age (± 4 years).
Participants: Data from 19 case patients and 76 controls were analysed.
Main outcome measure: The primary end-point was recurrence of heterotopic ossification. Secondary end-points were postoperative complications and, more specifically, sepsis that required surgical revision.
Results: There was no difference between the odds ratios (OR) for recurrence for each group (OR case group = 0.63, OR spinal cord injury subgroup = 0.45 and OR head injury subgroup = 1.04). The rate of sepsis requiring surgical revision was significantly higher in the case group (p < 0.05).
Conclusion: Based on the results of this case-control study, we suggest that radiotherapy should not be combined with surgery in patients with troublesome hip heterotopic ossification undergoing excision. Radiotherapy does not appear to prevent recurrence and, moreover, it is associated with an increased risk of postoperative sepsis.
Key words: heterotopic ossification; radiotherapy; recurrence; spinal cord injury; traumatic brain injury; excision.
Accepted Apr 23, 2020; Epub ahead of print May 18, 2020
J Rehabil Med 2020; 52: jrm00066
Correspondence address: Thibaud Honore, U1179 INSERM, Université Versailles Saint Quentin en Yvelines, UFR des Sciences de la Santé – Simone Veil, 78170 Montigny le Bretonneux, France. E-mail:
docteurhonore.thibaud@gmail.fr
The aim of this study was to evaluate recurrence and early postoperative complications following surgical excision combined with radiotherapy for troublesome hip heterotopic ossification in patients with spinal cord injury and traumatic brain injury. Data from patients in BANKHO database with spinal cord injury or head injury who underwent surgical excision of hip heterotopic ossification were included. Case patients underwent excision plus radiotherapy and controls only underwent excision. The primary end-point was recurrence. Secondary end-points were postoperative complications and, more specifically, sepsis that required surgical revision. Data from 19 case patients and 76 controls were analysed. There was no difference between groups regarding recurrence rate; however, the rate of sepsis requiring surgical revision was higher for patients who received radiotherapy. Based on the results of this study, we suggest that radiotherapy should not be combined with surgery in patients with troublesome hip heterotopic ossification.
Heterotopic ossification (HO) is defined as lamellar bone formation in non-osseous tissues (1, 2). It occurs particularly in muscle and connective tissue, and is often triggered by a lesion to the central nervous system (CNS). There is currently no consensus regarding its management. Administration of non-steroidal anti-inflammatory medication (NSAIDs) within the first 3 weeks of the neurological lesion decreases the rate of occurrence of HO (3); however, their use is limited by potential adverse effects (4, 5). Bisphosphonates were once considered as a promising treatment, but are no longer used due to the risk of rebound effects following cessation (recurrence after discontinuation of drug therapy). Furthermore, they cannot be administered until ossification is in progress (6).
Surgical excision of HO is the current reference treatment (2, 7, 8). It is generally accepted that excision should be carried out as soon as the HO becomes troublesome, i.e., causes pain or reduces function (9). The main complication of excision is recurrence (7, 10). Like the initial HO, the symptoms of recurrent HO may be sub-clinical (only seen on X-ray), may limit range of motion without affecting function, or may cause severe restrictions to function (10).
The rate of postoperative recurrence has rarely been evaluated, and a unanimous definition of recurrence is lacking in the literature (11–14). From the 1970s to the 1990s, recurrence rate in spinal cord injury (SCI) was diagnosed radiographically to be between 82% and 100%, but only 17–58% of HOs were associated with clinical signs (6, 10, 11, 15). In traumatic brain injury (TBI), recurrence was estimated to be 20% (16). Existing data suggests that the time between surgical excision and recurrence is the same as for initial HO after CNS injury: between 3 and 6 weeks (10), although it can be up to 3 months (17, 18). Contrary to previous beliefs, it has now been established that early surgery is not associated with recurrence of HO (9, 18–20). In a study of 357 patients (570 HO excisions), Genet et al. found no association between post-surgical recurrence and aetiology, sex, age or the presence of multisite HO. Furthermore, recurrence was not associated with the time elapsed between the CNS lesion and surgery. None of the 181 patients studied, all of whom underwent surgery in the first year after their accident, experienced recurrence during follow-up (7). A systematic review that assessed combined treatments for HO to prevent recurrence in patients with SCI or TBI (21) could not draw any conclusion about the effectiveness of any treatments, since all of the studies were either case series or retrospective studies with small patient samples.
The prophylactic effect of radiotherapy on development of HO has been well-described following orthopaedic surgery (22–24), but its effect on HO in patients with neurological disorders is less well-documented (2). It is believed that radiotherapy blocks mesenchymal stem cell differentiation into osteoblasts and bone precursor cells (11). Although radiotherapy is sometimes used, no studies have evaluated its effectiveness in patients with SCI and TBI to prevent recurrence of HO.
Radiotherapy can be used either in the initial phase of development of HO (25–28) or to prevent recurrences following surgical excision (26, 27, 29). Meiners et al. (30) evaluated the association of surgical excision and postoperative radiotherapy, and found a decrease in recurrence rate with radiotherapy. However, the study did not report the doses and techniques used, the indications for radiotherapy, or patient selection criteria.
Several case reports (6 patients in total) have been published, in which radiotherapy was administrated as a first-line treatment for large HOs (25, 31, 32). The results showed a reduction in pain and an improvement in joint mobility for several months following the radiotherapy. Sautter-Bihl et al. evaluated the effects of radiotherapy on progression and recurrence in patients with SCI during the inflammatory phase of HO development and after surgical resection of the HO (26, 27). They found that, in over 70% of the patients, HO development stopped following treatment. However, interpretation of the results is limited by the lack of homogeneity of the doses and fractionation protocols used. Finally, a retrospective case-control study reported that standard doses of radiotherapy did not reduce the recurrence rate (29).
The aims of this retrospective study were: (i) to assess whether radiotherapy associated with HO excision decreased post-excision recurrence of HO in patients with TBI and SCI and troublesome hip HO, and (ii) to evaluate the risk of associated post-operative complications.
This was a single-centre, case-control study of data from the BANKHO database (Raymond Poincare hospital, Garches, France). This design was chosen based on published guidelines for epidemiological studies of this type (33), i.e. the retrospective nature of the analysis and the small number of eligible records in the database from patients who had undergone radiotherapy.
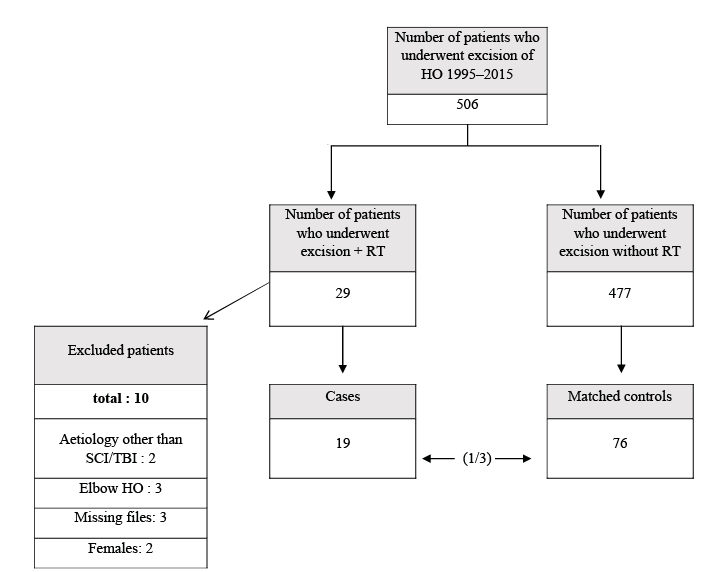
The BANKHO database contains all demographic, clinical and surgical data from patients who underwent surgical removal of HO following CNS injury since 1993 at our hospital. Indications for the surgical excision of HO were: (i) a loss of range of motion affecting function, (ii) pain or (iii) nervous or vascular compression. All surgeries and immediate postoperative evaluations were performed by the same orthopaedic surgeon. At the time of writing, 417 patients were listed in the database, including 609 initial surgical resections of HO. The flow chart of patients included in the present study is shown in Fig. 1.
The inclusion criteria for the present study were: patients in the BANKHO database with TBI or SCI and who had undergone surgical excision of hip HO.
The case patients had undergone HO excision, but, in addition, they had also received perioperative radiotherapy on the operated area. For the majority of case patients, the radiotherapy involved a single preoperative session, at a dose of 7.5 Gy, with 15 or 18 MV X-ray photons (carried out the day before surgery). Each case patient (excision + radiotherapy) was paired with 4 control patients (excision only). The controls were selected according to predefined matching criteria: aetiology (SCI or TBI), sex and age (±4 years). All the patients were operated on and followed-up in the same surgical department. All patients included were admitted between 1995 and 2015. Demographic and clinical data were collected for case and control patients.
The primary outcome measure was recurrence of HO. Recurrence was defined as being troublesome, i.e. affecting sitting or gait due to pain or reduction in joint range of motion. Radiological recurrence, in the absence of clinical signs, was not considered. Secondary outcome measures were postoperative complications of all types and complications that required revision due to sepsis.
Analysis of data in the BANKHO database was approved by the Committee for the Protection of Individuals. The study was non-interventional and routine procedures were used (i.e. no additional diagnostic procedures or medical supervision).
Statistical analysis was carried out using Sigma Plot software version 12.5. The effect of radiotherapy on recurrence was tested using a χ2 test (or a Fisher’s exact test when necessary) and then by a multivariate logistic model. The variables used for matching (sex and age) were the dependent variables. Adjusted odds ratios (OR) were calculated with 95% confidence intervals (95% CI). This was done for the entire sample and for the SCI and TBI groups.
Fig. 1. Study flow chart. HO: heterotopic ossification; RT: radiotherapy; SCI: spinal cord injury; TBI: traumatic brain injury.
Main results
A total of 29 patients in the BANKHO database underwent perioperative radiotherapy. Of these, 10 did not fulfil the inclusion criteria (see flowchart; Fig. 1). The case group was composed of data from 19 male patients. These 19 patients were matched with 76 control patients, all of whom also underwent HO excision without radiotherapy. Although the case and control groups were comparable with regard to certain characteristics (e.g. age at initial lesion, lesion level, ASIA score), there were also differences in the proportions of patients with multisite HO (case: 68.4% vs control: 35.5%), and recurrences after the first excision that required surgical revision (case: 78.9% vs control: 5.3%).
Finally, the groups differed in terms of time from CNS lesion to first HO excision (12.6 vs 18 months). The difference in time from surgery to recurrence (19.3 vs 51.7 months) could not be analysed due to the low number of recurrences in the control group (4 vs 15). Of the 95 patients whose data was analysed, 55 had SCI and 40 had TBI, and the recurrence rate was 14.7%. Of these, 29.5% had postoperative complications and 22.1% needed surgery for the management of these complications.
Table I describes the demographic data for both groups (case and control).
Table I. Patients’ characteristics
Radiotherapy treatment details
Only 21.1% of case patients received radiotherapy at the time of the first surgical excision. In the other patients of case group, radiotherapy was performed at the time of recurrence surgical excision. Most radiotherapy was performed preoperatively (89.5%), for logistical reasons. The protocol was one dose of 7.5 Gy in a single fraction (as recommended in the literature (34)). This was performed in 94.7% of cases. Detailed characteristics of the case group are presented in Table II.
Table II. Detailed characteristics of the case group
Results for radiotherapy group (n=19)
Symptomatic recurrence occurred in 10.5% of the case patients (n = 2). Almost half of these patients (n = 9, 47%) developed complications after surgical excision and radiotherapy, requiring surgical revision. It was always due to postoperative sepsis. Revision was carried out at a median of 28 days following excision. The mean follow-up time for this group was 11.7 months.
Results for control group (n=76)
Symptomatic recurrence occurred in 5.3 % of the control patients (n = 4). Almost one-third of these patients (n = 23.3%) developed complications after surgical excision and 21% (n = 16) required surgical revision, due to postoperative sepsis. Revision was carried out at a median of 27 days following excision. The mean follow-up time for this group was 25 months.
The results of the 2 groups are presented in Table III
Table III. Results for radiotherapy and control groups
Univariate analysis
Univariate analysis revealed no significant relationship between radiotherapy and recurrence of HO (odds ratio (OR) 0.63, 95% CI: 0.06–3, 27; p = 0.72). Equally, no correlation was found between radiotherapy and postoperative complications (all complications pooled) (OR 2.7, p = 0.056). However, there was a significant correlation between radiotherapy and sepsis that required surgical revision (OR 4.70, 95% CI: 1.38–16.26, p < 0.05). In the TBI subgroup, this relationship was not significant (OR 4.00, p = 0.13, 95% CI: 0.45–33.39) but it was significant in the SCI subgroup (OR 5.19, 95% CI: 1.04–27.90, p < 0.05). The results of the univariate analysis, for the primary and secondary outcome measures, for the total population (SCI + TBI) as well as the subgroups, are presented in Table IV.
Multiple logistic regressions for the primary outcome measure
There was no significant relationship between radio-therapy and incidence of recurrence, even when the matching variables (age and sex) and subgroups (TBI and SCI) were considered. These results are presented in Table V.
Table IV. Results of the univariate analysis for the primary and secondary outcomes
Table V. Results of the multiple logistic regression on the main outcome (recurrence)
Main results
This study did not find any relationship between radiotherapy administered at the time of HO excision and recurrence in patients with CNS disorders. Moreover, postoperative complications occurred more frequently in patients who underwent radiotherapy, particularly those with SCI.
Radiotherapy and HO
These data concurred with a previous case-control study by Cipriano et al. (29), which did not support the use of radiotherapy for the prevention of HO recurrence after excision in patients at risk of recurrence. However, a recent retrospective study suggested some effectiveness of radiotherapy to treat HO (28). Patients with SCI underwent twice-weekly ultrasounds to screen for HO, followed by magnetic resonance imaging (MRI) or computed tomography (CT) scans if HO was suspected. If diagnosed, a single dose of radiotherapy (7 Gy) was administered. Only 5.3% of the patients treated with radiotherapy experienced progression (presence of clinical signs) of HO, requiring further radiotherapy; however, the mean follow-up time was only 89.4 days (standard deviation (SD) 76 days) after the initial radiotherapy. Moreover, the spontaneous progress of HO is currently unknown (i.e. it is unclear how many HO cases would have remained sub-clinical and how many would have gone on to become “troublesome”).
In the future, one of the main challenges for the management of HO will be to understand the pathophysiology of its development. An important question is to determine whether HO seen on imaging will be likely to go on to become symptomatic and troublesome. One problem when reviewing literature on the prevalence of HO is the heterogeneity of sample characteristics in the publications. In studies of surgical intervention, HO tends to be troublesome, and thus excision is indicated. In medical studies, however, HO is often discovered by imaging (systematic screening by ultrasound) and confirmed by either CT or MRI scans (28, 35)) without having been first described as troublesome.
Infectious complications
The results of the present study suggest that prophylaxis by radiotherapy is more effective for patients with SCI than for those with TBI. However, the risk of sepsis (a postoperative complication requiring surgical revision) is elevated for patients with SCI. Patients with SCI are generally at a higher risk of infection due to pressure sores, chronic bacteriaemia, immunosuppression, etc. There is little data in the literature regarding acute, radiotherapy-related complications in SCI. In one study of patients who underwent total hip arthroplasty, with radiotherapy administered pre- or post-operatively to prevent HO, reoperation was required in 9% (removal of painful haematomas and explanation of an infected prosthesis). There was no difference in rate of reoperation between those who underwent pre- or post-operative radiotherapy (36). However, this data cannot be extrapolated to patients with CNS lesions.
Gatin et al. (37) recently demonstrated that a higher American Society of Anesthesiologists (ASA) score, younger age, and spinal cord injury as the cause of HO at the hip are risk factors for post-operative infection (POI). The proportion of patients with POI after hip HO excision was 10%, in accordance with previous reports.
Oncological risk
Radiotherapy is associated with an increased risk of cancer, although according to the literature, the risk is very low (38–40), particularly following a single radiotherapy session at a dose of less than 30 Gy (41). The follow-up duration in this study was not long enough to assess this risk; however, precautions were taken, as recommended by Seegenschmiedt et al., to protect the organs with the highest risk (bladder, rectum and colon) using lead shields (42).
Study limitations
The lack of significance regarding the effect of radiotherapy for the prevention of HO could be due to recruitment bias or a lack of statistical power. It is reasonable to assume that selection bias occurred, since the patients who underwent radiotherapy had the characteristics of patients in whom HO typically recurs: post-excision recurrence had occurred in 78.9% of the patients who received radiotherapy compared with only 5.3% of the patients in the control group.
Multisite HO was also more common in the case group than the control group (69% vs 36%) although this is not a currently recognized recurrence risk factor (7). Time from CNS lesion onset to initial surgery also differed between groups, although this is also not known to be associated with an increased risk of recurrence (16, 18). These differences could be attributed to the fact that surgery was a higher priority in the case group because of the presence of multi-site HO. Patients most at risk of recurrence were selected upstream based on empirically recognized risk factors (neurogenic bladder and pressure sores for patients with SCI, autonomic dysfunction in patients with TBI and SCI), or because they had already experienced post-surgical recurrence. Because this was a retrospective study, there was no blinding, and patients with a higher risk of recurrence were prescribed radiotherapy, similarly to the study by Cipriano et al. (29).
Another possible limitation is the long inclusion period, from 1995 and 2015. During this period, a single surgeon performed all HO excisions; however, the prophylactic antibiotic regimen was changed in May 2007 due to the high rate of POI (10%). No differences in POI frequency were found in the current study for surgery carried out before and after the change in antibiotic regimen.
Conclusion
Based on the results of this small case-control study, we would not recommend radiotherapy to prevent recurrence of HO in patients with troublesome hip HO, requiring surgical excision who are at high risk of recurrence. Not only does radiotherapy appear to be ineffective in preventing recurrence, but it is also associated with an increase in postoperative complications, particularly sepsis.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize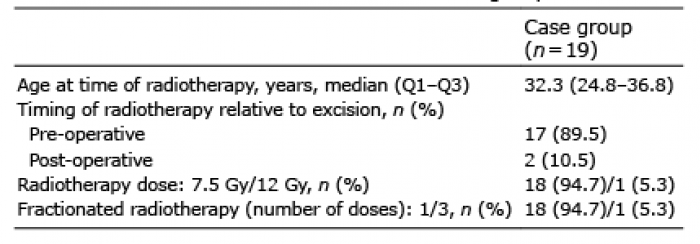 Click to show fullsize
Click to show fullsize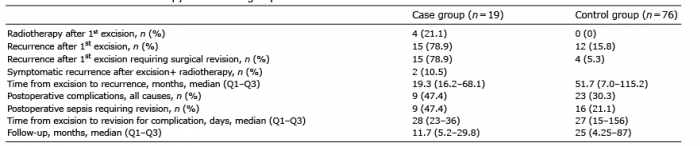 Click to show fullsize
Click to show fullsize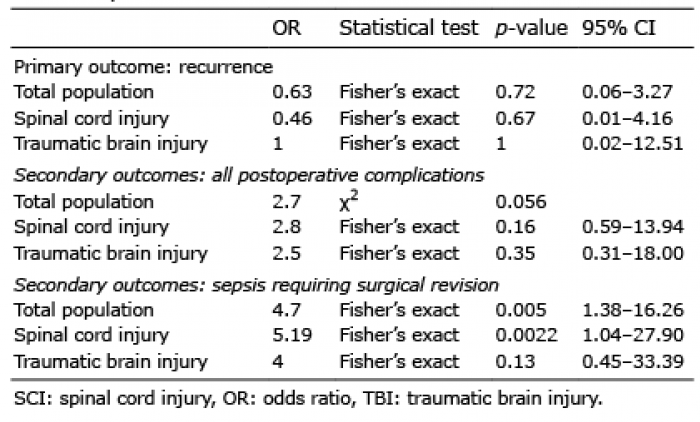 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize